
In an evolving health landscape, emerging research continues to highlight concerns that could impact everyday wellbeing. Here’s the key update you should know about:
A UK trial shows drones can deliver defibrillators faster than ambulances, but survival depends on better dispatcher guidance and bystander confidence in using the life-saving devices.
Study: The use of drone-delivered Automated External Defibrillators in the emergency response for out-of-hospital cardiac arrest. A simulation study. Image credit: EEs sarawuth/Shutterstock.com
Drones can capture breathtaking photos, patrol and monitor sensitive or dangerous areas, and deliver medical equipment or medication. One such use is to provide automated external defibrillators (AEDs) to help resuscitate cardiac arrest patients before they reach the hospital. A recent paper in Resuscitation Plus examines how drones help in this emergency response.
Introduction
Nine out of ten people who suffer an out-of-hospital cardiac arrest (OHCA) die before being discharged from the hospital or within 30 days of the arrest. The chances of survival and of neurological recovery are doubled if bystanders can provide prompt cardiopulmonary resuscitation (CPR) and use an automated external defibrillator (AED) to get the heart beating again.
The issues with bystander AED defibrillation include not being able to find, access, and retrieve an AED from a public location. In an earlier study, only 5%- 22% of people knew where to find the nearest public AED. Many AEDs are difficult to reach (up to 59%), and only 3%- 25% of OHCAs occur in the vicinity of an AED.
Drones could reduce the time required to get an AED to the OHCA patient compared to an ambulance. Drones are also user-friendly. The authors of the current study have already demonstrated these aspects in their earlier research.
However, that study showed that call handlers needed more support. The present study sought to understand the chief problems reducing the effectiveness of bystander AED use on the OHCA scene.
About the study
The researchers simulated an OHCA scene beginning with a call to 999 for emergency help. This was followed by the dispatch of a drone that could perform autonomous flight “Beyond Visual Line of Sight” (BVLOS) to the location of interest.
The drone operator was in touch in real time with the call handler, passing on the drone’s progress. Participants were recruited for the capability to perform CPR or use an AED outdoors, but recent training varied, and many struggled with AED use. Only 64% had CPR training in the past five years, and just 36% had AED training. The experience was assessed using video recordings, audio recordings of the emergency call, and post-simulation interviews.
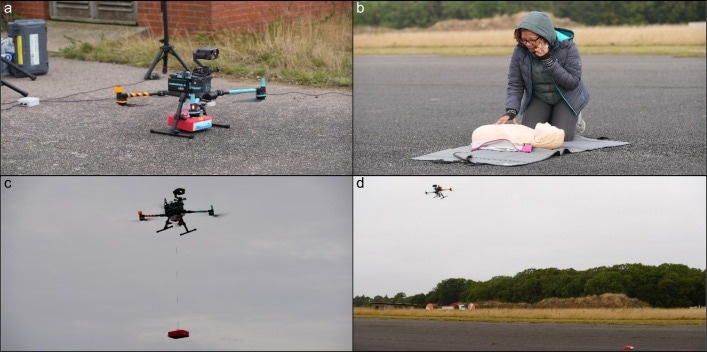
a) drone at remote site with AED loaded, b) emergency call made (study team member shown), c) drone on-scene winching AED to ground, d) drone departs and bystander informed it is safe to retrieve AED on ground.
Study results
Out of 11 single-bystander OHCA simulations, most participants were male with a median age of 62. Only one had used an AED in real life to help an OHCA patient.
An AED was delivered on nine occasions by drones. The median simulation time was 9:13 minutes, from placing the emergency call to resuming CPR after delivering an AED shock.
The call to allocation took a median of 1:28, allocation to take-off 0:49, and call to take-off 2:18. The first shock was delivered after another 4:35 minutes (median) from when the drone arrived at the scene. This was while the AED was being winched down, disconnected from the winch, and the subsequent departure of the drone. This was the “safe to approach AED” point, when the would-be rescuer left the patient to retrieve and bring the AED to the patient.
This meant a hands-off period (when the patient did not receive CPR) of 2:32 minutes. Of this, 16 seconds went to retrieving and bringing back the device. The rest of this delay was in extracting the AED from the carry case, attaching it to the patient, and delivering the shock.
It was relatively easy to retrieve the AED device, and the sight or sound of the drone did not distract from CPR performance. Participants sometimes found it hard to hear the call handler clearly, especially as the drone approached. Moreover, this loss of clarity increased hands-off CPR time while the bystander tried to listen or clarify instructions about the location of the incident or the CPR procedure, for instance.
The most significant difficulty occurred when removing the AED from the carry case, which participants felt was unusual and challenging to use. Bystanders felt the AED winch was too slow and unnecessarily prolonged the wait for AED use.
Conflicting AED and call handler instructions created serious problems. The call handlers did not provide instructions specific to the device or monitor correct AED use. The bystanders did not hesitate to retrieve the drone, but were often not confident about using it. In fact, two bystanders did not attach the AED to the patient.
Conclusion
The study showed that autonomous BVLOS flights of an AED-carrying drone to a simulated OHCA scene are feasible. The observations show how the pilot-call handler conversation delivers timely help to the site through the AED. However, bystanders often struggle to manage the call handler’s instructions and CPR.
The drone was deployed rapidly, but there was an additional delay at the scene: about 4.35 minutes from arrival to deliver the shock. This led to a total CPR stoppage of 2.32 minutes.
“Bystanders and call-handlers need more support to effectively use drone-delivered AEDs.” This aspect of call-handler training should receive as much or more attention as AED delivery itself. Call-handlers are often unsure how far CPR may be paused and how to help the bystanders use the AED.
The authors focused on a single-bystander scenario; given that only 16 seconds were spent away from the patients to fetch the AED, this use case may be acceptable.
Most importantly, studies must show that such interventions improve patient survival. Further research is needed in multiple fields, including how to integrate drone-delivered medical equipment into local emergency medical services and script responses for a more standardized help protocol, especially considering the need to guide bystanders in AED use.
Key limitations include operational challenges such as weather and technical cancellations, connectivity failures that forced the auto-returns, and the slow AED winch design. Regulatory approval and safety oversight, such as from the UK Civil Aviation Authority, will remain essential.