

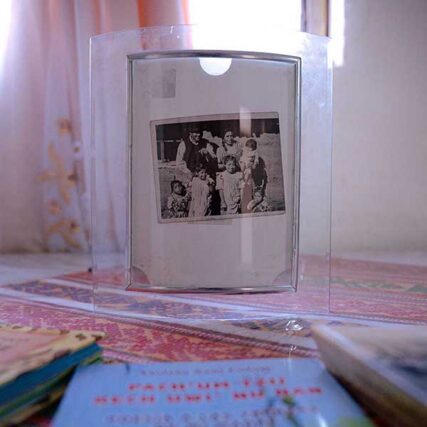
In the mountain town of Quetzaltenango, Guatemala, on the second floor of Ada Violeta Chuc’s home, a room with faded cream-colored walls holds an altar to honor her family’s ancestors. A wooden cross stands in the center of a table covered by a tablecloth printed with red poinsettias. A dozen figurines of Indigenous and Christian deities, along with candles, water, incense and other offerings surround the cross.
On the wall behind the table hang photos of seven deceased relatives. Four died of cancer.
“The one at the top is my grandma, my mother’s mom; she died of stomach cancer,” Chuc recently told a reporter from the International Consortium of Investigative Journalists. She pointed at the frames as she spoke. “My mom’s cousin also died of uterine [cancer]. And this is my mom’s sister; she died of colon cancer. She was only 23.”
The photo in the center of the gallery is the most recent addition: Chuc’s mother, Francisca Violeta Sam Colop, who died in July 2025 after a long journey with skin cancer. In the photo, Sam Colop, an Indigenous Maya K’iche’ educator from the Guatemalan highlands, is smiling widely, sitting with crossed arms, wearing a traditional handwoven blouse, or huipil, with blue, green and purple embroidery.
“There is always the fear that [cancer] might strike me, strike one of us next,” Chuc said. “There is so much you can’t control.”



One night in 2012, Chuc said, Sam Colop noticed a stubborn dark spot on her right foot. She shrugged it off, telling her daughter it was a mole. But a dermatologist diagnosed her with melanoma. For the next nine years, Sam Colop was in and out of hospitals, undergoing surgeries and enduring round after round of chemotherapy. Still, the tumors kept spreading.
In 2021, she visited one of the country’s top oncologists, who prescribed what he considered to be the most effective treatment: pembrolizumab, an intravenous immunotherapy drug known as Keytruda. After its approval by the U.S. Food and Drug Administration in 2014, Keytruda began selling in the United States, Europe and Japan but was less available in developing countries like Guatemala.
Sam Colop would need regular infusions, and each cost nearly $11,000. “The whole treatment costs millions of quetzals [hundreds of thousands of U.S. dollars]. It would be impossible to afford,” Sam Colop’s husband, Juan Chuc Xum, recalled one doctor saying.
Sam Colop had to fight to get the medication, eventually taking her country’s publicly run health insurance system to court. By then, she’d been living with cancer for over a decade.
“Could [Keytruda] have saved my mother’s life?” Chuc wonders. “I think it would have. I also believe it was too late when she got it.”


Sam Colop’s case is similar to that of thousands of patients around the world — particularly those in developing countries — who have taken on draining bureaucratic battles with public and private insurers to access Keytruda, which can cost anywhere from about $29,000 in Indonesia to $130,000 in Colombia, to $208,000 in the United States for a year of treatment. In developing countries, the drug is rarely included on the national lists of essential medicines, which governments rely on to decide what public and private insurers must cover. As a consequence, insurers in some low- and middle-income countries largely avoid covering the drug unless a court or regulator forces them to. Some cancer patients have died while waiting for health systems to comply with court decisions. Others have paid thousands of dollars out of pocket before their insurers complied with courts’ or regulators’ orders.
In South Africa, one of the only countries in sub-Saharan Africa where Keytruda is readily available, a small-business owner who has lung cancer can’t get her private insurer to fully comply with a landmark ruling by the national regulator to cover Keytruda. In Guatemala and elsewhere in Latin America, patients like Sam Colop have taken to courts to force their insurers or public health systems to provide the drug. Patients in wealthier countries struggle for access, too: In the United States, a CEO of a medical consulting firm went without treatment for many weeks while fighting a denial of coverage of the drug.
Many high-cost drugs trigger court battles. But Keytruda — which has made around $163 billion in revenue for Merck & Co. since its launch more than a decade ago — is one of the starkest symbols of a dysfunctional global system that disproportionately hurts poorer countries with limited health care budgets and little negotiating power with Big Pharma.

These findings are part of the Cancer Calculus, an investigation by ICIJ and 47 media partners that examines the reasons for Keytruda’s exorbitant prices — and exposes the global consequences.
Speaking in part to those consequences, Merck told ICIJ: “We operate in compliance with the applicable laws, and regulations, and do not support, promote, or engage in any activities intended to encourage legal claims. While legal claims are a lawful administrative pathway for some patients to access medicines, we believe they are not a sustainable approach, since it may be an inefficient use of government budgets, and do not consistently enable timely, predictable, and broad patient access.”
The company said that the development of Keytruda “is now one of the largest and costliest pharmaceutical [research and development] programs ever undertaken.”
Merck also said: “We have a long history of responsibly pricing our medicines to reflect their value to patients, payers and society. To ensure our products reach as many patients as possible, we price them differentially across markets, and sometimes within markets, according to numerous factors. These factors include the value a therapy brings to patients and the healthcare system, countries’ pricing and reimbursement systems and the ability of governments to finance healthcare.”
But, as Daniel W.L. Wang, a law professor at the Fundação Getúlio Vargas in Sao Paulo whose research focuses on health-related litigation in Latin America, explained to ICIJ: “Many of these countries are middle- or low-middle-income countries, and they struggle to universalize even the most basic health services. So the claims for pembrolizumab put a lot of pressure on their health budget.”
“Even if we improve the funding for our health system, even if we improve our policies, this is still a cost challenge,” he added, “because the cost of the treatments grows at a pace that the health systems budgets cannot keep up.”
As a result, a sky-high price of a potentially lifesaving cancer drug puts it out of reach for many health systems, forcing patients who have the resources — and stamina — to fight for the right to treat their disease. When this happens, access to pricey drugs can become less about medical need and scientific evidence and more about whose lives are worth saving.
‘The judicialization of health care’
By the time Sam Colop was diagnosed in 2012, her family had moved from a modest home on the outskirts of Quetzaltenango to a nicer two-story house near the town’s center, a sign of upward mobility seldom achieved by Mayan families. Sam Colop worked as a teacher, then principal of a bilingual Spanish and K’iche’ school, and as a college lecturer, allowing her to access Guatemala’s publicly administered insurance program, the Instituto Guatemalteco de Seguridad Social (the Social Security Institute), known locally as IGSS.
The IGSS is funded by mandatory payroll deductions and covers more than 3.3 million people. To receive care, beneficiaries must use designated IGSS hospitals and doctors. Patients who require faster, specialized care usually seek out private hospitals, paying out of pocket or with supplemental insurance.

Over the years, Sam Colop underwent more than 30 surgeries in private hospitals, paid for with her salary and by selling her car and the piece of land her parents left her, Chuc said. For chemotherapy and targeted therapy treatments, she’d endure a grueling four-hour bus ride along the winding highway that connects Quetzaltenango with the capital, Guatemala City, to receive her medication at the IGSS hospital.
“I remember one time she had to go to Guatemala City for her treatment and she didn’t have the bus fare,” Chuc said. “A group from church came and gave her an envelope with a donation.”
Eventually, Sam Colop sought a second medical opinion from Eduardo Gharzouzi, an oncologist outside the IGSS system. A genetic test indicated she’d be a good candidate for Keytruda, Gharzouzi told ICIJ partner Plaza Pública.
But when Sam Colop requested that IGSS provide the medication, she didn’t get an answer. (IGSS has never included Keytruda on its official list of covered medications, and there are no biosimilars for Keytruda on the IGSS list.)
Out of options, the family paid a lawyer about $1,300 to file an amparo. This distinctively Latin American legal remedy, similar to an injunction, protects constitutional rights — like health and life — from abuses by the state and, sometimes, private entities. It was implemented in Mexico in 1857 and inspired many other Latin American countries to adopt similar protections, under the name amparo or tutela. Each country has its own rules about who can use the injunctions and which rights they protect.
“The amparo is the right of every person to appeal to a court in the face of an arbitrary act or the violation of another right,” Jordán Rodas, a lawyer and former human rights ombudsman in Guatemala, told ICIJ. “Ideally, however, people wouldn’t have to resort to legal protection to guarantee their health care.”

Access to costly health care is a common reason to file amparos, with patients asking judges to force insurers and public hospitals to provide expensive medication and treatment. While amparos or tutelas are the go-to legal mechanism to seek access to expensive medication in many South and Central American countries, in Brazil most patients file regular lawsuits, explained Wang. Fewer patients seek the treatments through mandados de segurança, Brazil’s version of the amparo, he added.
Researchers who have analyzed the phenomenon in Brazil and other South American countries, including Wang, have dubbed it “the judicialization of health care.”
“The courts in Central and South America treat the right to health as an absolute individual right,” Wang said. “So as long as you can show that you need the treatment, no matter the impact on the health system, no matter the impact on the other users of the health system, you have the right to receive it.”
Data analyzed by ICIJ shows that health and legal systems are increasingly intertwined in some Latin American countries, where Keytruda is often accessed through a court order. In Guatemala, from December 2022 to February 2026, the Constitutional Court — Guatemala’s highest court for constitutional matters — examined 96 amparo petitions for Keytruda coverage; all but one were granted.
In Brazil, federal and state courts have examined around 4,300 judicial requests for pembrolizumab since 2019; the majority ruled in favor of patients. In Mexico, ICIJ partner Quinto Elemento Lab found 55 amparos filed from October 2017 to February 2026. Thirty-six of those granted access to Keytruda, and eight were dismissed because the drug was provided to the patients before the courts had to decide. And in Chile, courts sided with patients in 10 of a dozen cases.
Nearly all of the amparo petitions in Guatemala were filed by IGSS beneficiaries. The IGSS has provided Keytruda to patients since at least 2018 — but generally after being forced by courts, public records show.

In a statement to ICIJ, IGSS said that high-cost medications “are administered under technical and medical protocols designed to balance timely access, available scientific evidence, and the sustainability of the system.”
“In this context, the IGSS has allocated significant resources to provide these types of treatments, amounting to approximately 1,703 million quetzals [more than $218 million] — a figure that reflects the growing demand and the progressive incorporation of specialized therapies,” the statement said. “The institution implements evaluation processes for the inclusion of new treatments, prioritizing patient safety, therapeutic efficacy, and the rational use of public resources.”
Sam Colop’s amparo petition argued that her IGSS-sanctioned treatments — chemo and targeted therapies — hadn’t stopped her disease’s progression. In May 2021, a court ruled in her favor, and she began receiving Keytruda. IGSS appealed the decision, arguing that it hadn’t denied Sam Colop comprehensive medical care and raising concerns about more than 30 possible side effects of Keytruda.

In court records reviewed by ICIJ, the public insurer said in its appeal that it had “no legal obligation” to buy specific commercial brands. According to IGSS’ arguments, the judges were overreaching by making decisions that should be left to “medical professionals within the scientific sphere of medicine.”
The case reached the Constitutional Court, which sided with Sam Colop in September 2021, four months after the original court decision in her favor. The ruling ordered IGSS to continue to provide the medication as prescribed and ensure there is no shortage of the drug.
For two years, Sam Colop received Keytruda when it was available. Medical supply shortages are common in Guatemala and other Central American countries due to underfunding of health systems and a high reliance on imported medication. Chuc recalled several times when Sam Colop traveled to the capital to receive her infusions, only to find out there was no medication. During these shortages, she’d go back to chemotherapy or miss treatment altogether.

The IGSS said in its statement that it “operates under principles of equity, legality, and transparency, utilizing internal procedures that allow for the review of clinical cases and the processing of requests in accordance with medical and administrative criteria.” Regarding judicial rulings, IGSS said, “in cases where a final judicial ruling mandates the provision of a specific medication or treatment, the institution is required to comply faithfully and strictly with said mandate.”

By 2024, Sam Colop was in a wheelchair. The cancerous tumor on her right foot had become a deep, open sore, and her cartilage was nearly exposed. That April, though, she received good news and texted her family’s WhatsApp group: “the medication is back! I’m going back to my immunotherapy.” But by then, the off-and-on schedule had seemingly taken its toll; after two infusions with a different immunotherapy combination, her health began to rapidly decline.
In anticipation of her death, Sam Colop reminded her daughters to follow her detailed instructions for a burial according to Mayan faith: They were to dress her in the green huipil she wore to celebrate her 60th birthday and include incense, her comb, and her mirror in her coffin. On a warm afternoon last July, Sam Colop’s daughters and the oldest of her seven grandchildren were sitting around her bed when she died. “She opened her eyes widely,” Chuc said, “as if she wanted to look at us one last time.”
‘A choice between survival and solvency’
Thousands of miles across the Atlantic Ocean, in the port city of Durban, South Africa, Adri Jeffers, a 57-year-old owner of a small clothing label and mother of three, is embroiled in her own battle over Keytruda. Jeffers — stylish and businesslike with jet-black hair and thick-framed spectacles that accentuate her angular features — has top-tier private health coverage. Her fight led to a draining legal process, too, this time before a regulatory body for health insurance.
Like Sam Colop, cancer runs in Jeffers’ family. Her mother lived with breast cancer for many years before she died, and her father died of lung cancer. Still, when Jeffers was first diagnosed with Stage 3 breast cancer in 2005, at age 36, it came as a “massive shock,” she told ICIJ at her two-story Victorian home.
The diagnosis, she said, was “a life-altering moment — not something you consider in your 30s whatsoever.” She tried to stay positive around her then-9-year-old twins and 3-year-old son, but the strain was constant: “They’d look at you very bravely, but then you would walk past their room later and hear them crying. … Internally you’re basically crumbling, but you [act tough] so as not to upset the kids and your husband.”

After chemotherapy, remission, then a resurgence in 2007, Jeffers kept the cancer in check with vigilant monitoring and carefully managed treatment. But in 2015, she was overtaken by a strange fatigue and weakness. One night at a restaurant, she turned to her husband and said, “I think it’s back.” She was right. Scans showed that the disease was spreading again.
She started what she calls a standard treatment plan, involving rounds of chemotherapy. At times the treatment felt worse than the disease. “She would deflate like a balloon in front of your eyes” and be bedridden for days, said her husband, Wayne. Jeffers tried to schedule her chemo sessions on Fridays so she could recover over the weekend.
Over time, her oncologist tailored her treatment, and for the next several years, Jeffers would “knock back the cancer a little bit, rest a little bit, and repeat,” she said.
But in 2023, a scan picked up a nodule in her right lung. She soon had a new diagnosis: primary lung cancer. It was spreading aggressively, and the usual therapies were no longer working.
The news took a heavy toll on her children, by then 26 and 21. Her youngest son “was unable to cope with the diagnosis,” she said, and left an internship in Cape Town early to be with his mother.
Jeffers’ oncologist suggested she was a strong candidate for Keytruda. Jeffers was aware of the drug; she’d seen the news of former U.S. president Jimmy Carter’s remarkable response to it.
In May 2023, Jeffers’ oncologist wrote to her medical aid scheme, Medshield, requesting coverage for a combination of chemotherapy and Keytruda. In South Africa, those able to afford private health care — a minority of the population — are typically covered through what are called medical aid schemes. These are regulated, not-for-profit medical funds, often administered by for-profit companies, that pay out claims from a pooled system of member contributions.
After Medshield declined her request, stating that Keytruda was not covered by her insurance plan, Jeffers — now familiar with the bureaucracy of insurance and with the help of her oncologist — appealed twice. Rejected, she lodged a special request for ex gratia coverage, meaning she appealed to Medshield to provide coverage out of a sense of moral obligation or goodwill. Before the year was out, Medshield had declined that request, too. Keytruda was not on South Africa’s essential medicines list, Medshield argued, and had not met the eligibility requirements for coverage of Jeffers’ cancer. Medshield also asserted that the mutations of Jeffers’ cancer made Keytruda clinically unsuitable — a claim that her oncologist strongly contested in a letter to the medical scheme.
Jeffers spent over four hours a week sending emails and following up with unresponsive Medshield staff, she told ICIJ. “The order of business [for insurers] is not to honor claims unless you [the patient] object, especially with oncology,” she said. “So once I figured that out, I understood you have to object and question.”

Her meticulous organization skills, honed by years of running her business, came in handy. Over the years, she has kept every record of her medical history: invoices, emails, letters, medical test results. Each item is archived, ready to be quickly summoned in her next dispute. “Not everyone has the tenacity and the circumstances to be able to do this,” she said.
As Jeffers’ fight dragged on, her health deteriorated. She’d been in the hospital five times in 2023.
She found a lawyer online who specialized in medical aid claims. On his advice, in the summer of 2024, Jeffers turned to South Africa’s statutory regulatory body for private health insurance plans, the Council for Medical Schemes. “I’d done what I needed to do: [had surgery to remove] the tumor, went onto chemo, and it failed,” she told ICIJ. “So I should be entitled to use immunotherapy.”
Keytruda is not on South Africa’s list of essential medicines largely because of its prohibitive cost, so it is not available in overstretched public health facilities that serve the majority of the population. (The price tag is nearly $5,000 for a typical 200 mg dose in a country where the median household annual income is only about $5,200.)
My struggle became not only against cancer, but against the very system meant to safeguard me.
— Adri Jeffers, small business owner and mother of three
Andy Gray, a senior lecturer in pharmacology at the University of KwaZulu-Natal in Durban, who is involved in medicines selection and regulation, said that “the essential medicines list is based on some sort of estimate of affordability as well as public health priorities.” Although this includes cancer drugs, these are “predominantly older, off-patent items where there’s either been a decision by the company to market a clone to the state at a different price or [it’s possible to] take advantage of new generic entrants. But in general, the number of monoclonal antibodies [like Keytruda] is severely limited, and that’s based mainly on their cost.”
South African courts have established the precedent of “progressive realisation” of the right to health, meaning that the government is obligated to take steps to improve access to health care and ensure the realization of the right, but within reason — resource constraints must be taken into account. While patients increasingly sue the state for access to medicines in some other developing countries, like Guatemala, the courts in South Africa rarely grant orders on constitutional grounds to provide high-cost treatments. There is little hope of uninsured cancer patients gaining access to Keytruda unless they can enroll in a clinical trial.
For the more than 9 million South Africans with private health coverage, disputes with insurers typically end up before the Council for Medical Schemes, a statutory body that regulates private health insurance schemes. The CMS’ rulings are binding and can only be overturned by a court. (When disputes between patients and insurers do go to court, they normally focus on contractual obligations and the law governing medical insurance, not the constitutional right to universal health care.)
Jeffers couldn’t afford to wait while her complaint ground through the official channels. She and her family decided to raise their own funds for Keytruda. The family could have set up an online fundraiser, but “I didn’t feel comfortable with it,” Jeffers said.
They had already successfully applied to a cancer support fund called the Access to Innovative Care Foundation, or AICF. The foundation helps patients in South Africa fund gaps in their coverage — when there are hefty co-pays for expensive cancer therapies, for example. But the AICF is supported by various Big Pharma companies — including Roche and Novartis — ostensibly to mitigate high prices, so it is “in some ways controversial,” said Paul Ruff, a medical oncologist and professor at the University of the Witwatersrand in Johannesburg. In South Africa, a statutory “single exit price” ensures that manufacturers and importers sell a product at a standard price to all private sector buyers and are prohibited from offering rebates, discounts and other such incentives. Ruff sees the AICF as a way around this regulation, effectively making drugs more affordable to some without having to lower prices.

The AICF declined to say which Big Pharma companies fund it but told ICIJ in a statement that it “assists in ensuring access to healthcare, where such access is hampered by reimbursement and financial challenges,” and that it “operates at an arms’ length basis from donors, guided by a Board comprising seasoned independent directors in the NGO sector, and renowned healthcare professionals, including oncologists.”
Merck told ICIJ in a written statement that it is “dedicated to making our medicines available to patients who may benefit from them as soon as possible — which is why Merck … provides many support programs and services to help ensure that people prescribed KEYTRUDA have access to our medicine.” Merck in South Africa, where the company is known as MSD, did not respond to questions about whether it funds the AICF.
In Jeffers’ case, the AICF agreed to cover half the cost of Keytruda, leaving her family to pay hundreds of thousands of rands out of pocket (about $85,000 currently) — and at a time when their income was drying up, as their business was still recovering from the shock of the COVID-19 pandemic and government restrictions. They were looking at having to spend roughly $2,450 at today’s price every six weeks for an infusion of Keytruda. They downsized their factory and sold off “scooters, sewing machines, fabrics, machines, computers, racking and shelving,” Jeffers’ husband told ICIJ.

Jeffers and her family scraped together the money by early 2024. Within months of starting Keytruda, Jeffers noticed dramatic improvements. The side effects were tolerable; she was regaining her strength. Her scans showed that her tumor was shrinking. “For the first time I thought I might actually survive this,” Jeffers said.
Still, the financial strain was crippling. Each month, Jeffers said, was “a choice between survival and solvency.” They anticipated 35 infusions of Keytruda prescribed by the oncologist — with half the cost covered by the AICF — and hoped for a favorable CMS ruling. After depleting their savings, Wayne Jeffers told ICIJ, “the plan was then to use her retirement annuity.”
In July 2024, Adri Jeffers finally received good news: The CMS ruled in her favor, laying out a detailed clinical assessment showing “well demonstrated” improvements in survival rates for people with her type of cancer and ordering Medshield to fund Jeffers’ Keytruda in full. The CMS went even further, stating that the ruling also applied to “all other members who are in a similar position.”
Jeffers was “blown away” by what she saw as “a groundbreaking proclamation” that was a victory for herself and other cancer patients. But after the ruling, Jeffers said, Medshield stalled, failing to meet its payment obligations despite her constant emails reminding them. “The stress in between [treatment and approvals] is enormous,” she told ICIJ, “because you know your clock is ticking, you know what the studies say, and you know you’ve got to keep up the treatment.”
A month after the CMS ruling, on Aug. 21, Jeffers received an email from a staff member at Medshield. She soon realized that, while it was about her, it was not intended for her. The staff member, she figured, must have accidentally copied her on internal correspondence. The communication, with Medshield discussing its decision to deny coverage due to Keytruda’s “exceptionally high cost and limited overall survival benefit,” was startling to read. “They were discussing how they weren’t sure about my survival — that they couldn’t guarantee survival because I had been on so many treatments,” Jeffers said.
Her husband said he was shocked “to see the value of her life being worked out on a page.”
Jeffers immediately sent the correspondence to her lawyer, deciding not to disclose to Medshield what she had seen for fear of some sort of legal consequence. In September, Medshield wrote to Jeffers to say that they would only reimburse her for what she had paid; they would not fund any further treatment. “But I had a ruling” from the CMS, she said. “For us it was trauma and disbelief.”
After Jeffers’ lawyer contacted Medshield, it agreed to continue funding Keytruda. But every victory felt temporary. In July last year, Medshield notified her that it would only cover further Keytruda treatments until November 2025 — at which point Jeffers would have had 16 sessions — far fewer than her full complement of 35. Jeffers said that the medical aid scheme backed down again, this time because she publicly criticized Medshield on social media.
Every day she braces for another hurdle. “My struggle became not only against cancer,” Jeffers told ICIJ, “but against the very system meant to safeguard me.”

In response to written questions from ICIJ, Medshield said: “Following careful consideration, including the evidence presented at the CMS hearing indicating, in contrast to available clinical studies, that the treatment has shown positive results, Medshield elected not to pursue an appeal and proceeded with compliance.”
Medshield said that it “acknowledges that intermittent delays occurred in the member receiving treatment due to previous technical errors in the claiming process, but this did not constitute a decline for the requested treatment or a withdrawal of the approved treatment regime.”
Medshield also highlighted the cost burden of expensive cancer therapies and the risk this poses to the sustainability of medical aid schemes that “are governed by legislation requiring them to accept all applicants regardless of prior health history and operate as not-for-profit entities that cannot access external capital.”
The rising costs of treatment and “open-ended funding” for that treatment, Medshield said, would have to be passed on to members. “Claims paid each year must be covered in full by premiums collected meaning there is no buffer against catastrophic oncology expenditure beyond premium increases.”
A treatment setback and a social media campaign
In the United States — the country with the highest drug prices and overall health care spending among developed nations — Tiffany Ferguson, like Jeffers, fears that the next message from her insurer will deny her coverage of Keytruda.
Ferguson, 42, was diagnosed with Hodgkin lymphoma in January 2019, after she started rapidly losing weight and experiencing violent coughing, vomiting and night sweats. “My doctor showed me the scan and said, ‘This isn’t good. You either have tuberculosis or cancer,’ ” Ferguson recalled. “I remember praying to God that it was tuberculosis.”
Years of treatments — including chemotherapy, a stem-cell transplant and targeted IV therapy — held the tumors back, but they returned in 2021.







In March 2022, her doctor, a hematologist-oncologist at the Mayo Clinic in Phoenix, about a two-hour drive from Ferguson’s home in Flagstaff, switched Ferguson to Keytruda. A few months later, Ferguson was in Phoenix, not far from the Mayo Clinic, sitting with her husband, Ryan O’Hara, in their Ford F-150 truck when she received a message from her oncologist. “Your scan looks great,” Ferguson read from her phone, her voice cracking. She couldn’t wait to break the news to her children.
After her first four treatments with Keytruda, she was in complete metabolic remission, the technical way to say there is no active cancer. “I remember sitting at the doctor’s office, looking at the clean scans [and thinking], I wish I had gone on [Keytruda] sooner,” she said.
Then one afternoon in July 2024, as she was sitting in the infusion chair, ready for her next dose, a staff member walked in and told her her insurance had denied further coverage. Ferguson knew that if she went ahead either she or the cancer center would be stuck with the $12,000 Keytruda bill, on top of other costs. “I was already poked, but I elected to stop and reschedule,” she said.
The insurance denial was the beginning of a bureaucratic process that set her treatment back eight weeks while Ferguson, her husband and her medical team exhausted nearly every option to fight the denial.
In the United States, it’s nearly impossible to know how many of the more than 220 million people with private health insurance are denied coverage for specific treatments. But an analysis of 2023 data by the health policy organization KFF found that 20% of claims to insurance plans sold through the government marketplace were denied, with fewer than 1% of denied claims appealed. And 56% of those denials are upheld.
Regarding Keytruda prices in the U.S., Merck said in a statement that what patients paid depends largely on their insurer. Slightly more than half of patients paid nothing per infusion, and those who paid were charged “between 1 cent and $375 per infusion, after satisfying their deductible” the statement said. It also said it provided about $125 million in co-pay assistance in 2025 and supported a charitable program that delivered more than $1.7 billion in free medicines to patients in the U.S. in 2024.
But when patients are denied coverage, their options are limited. If appeals to the insurer fail, filing a complaint with the state insurance regulator may be the last recourse. Depending on state laws, complaints to regulators may become public records. ICIJ requested complaints filed for denials of Keytruda from regulators in nine states. Two of those states provided information. ICIJ reviewed documents from Texas, which provided six final complaint resolutions, and in three of those the denial was reversed once it was reviewed by regulators. In California, an ICIJ examination of patient requests for independent medical reviews shows 17 cases upheld and 10 cases overturned.


Ferguson knows this system all too well. She is a medical social worker and the CEO of a small health care consulting firm that advises and trains hospital staff to handle case management, including insurance paperwork. “This situation blurred my personal life and my professional life,” she said. “Here I’m on the receiving end of this issue.”
In its denial letter dated July 17, 2024, CVS Caremark, the pharmacy benefits manager for Ferguson’s insurer, CareFirst BlueCross BlueShield, said it only covered the drug for 24 months for her “health condition.”
For Ferguson, the insurer’s argument “made absolutely no sense.” Keytruda has been the only treatment that has kept her in remission long-term, she said. Ferguson and her medical team found a recent study that they said showed the drug worked beyond the two-year period. “How could [the insurer] not be aware of this?” she wondered.
CareFirst BlueCross BlueShield did not respond to ICIJ’s requests for comment for this story.
Ferguson’s care team submitted documentation of the recent study. A doctor from a third-party advocate, PayerWatch, which was then her husband’s employer, helped file the appeal.
Ferguson and O’Hara spent countless hours on the phone and in front of the computer dealing with the insurer’s staff. Ultimately the insurer upheld the denial, rejecting both her appeals.
Ferguson was willing to go to court if necessary, she told ICIJ. But she and her husband felt the ultimate decision should be between Ferguson and her doctor, and so they tried another tactic, tagging the insurer publicly on social media. Ferguson, an occasional contributor to health care blogs and newsletters, wrote about her situation and talked about it on the podcast “Talk Ten Tuesday,” popular among health care professionals.
O’Hara wrote a long post on LinkedIn airing his frustrations with the process, without mentioning his wife’s name. “This isn’t how I like to use social media, but sometimes, as consumers, it is what we are left with. I do this for a living, and I would do this for anyone, but this one is also personal, as many of you know,” O’Hara wrote. “And, there are too many people out there not getting the care they need because insurance companies, not Doctors, dictate the delivery of care.”
Ferguson reposted it, writing: “Obviously this is very personal to me and I’m still trying to formulate my words. We are people that know the convoluted system. … Many people do not have access to such resources to understand work arounds for such a messed up system. Even with all the advantages, I am denied care — care that has kept my cancer in check and able to live a pretty ‘normal’ life.”
“I felt a bit exposed,” she told ICIJ about making her plight public. “I have shared my story before, but I have never made it my platform.”
After the post, she went about her day. “Life goes on, you have kids, dinner, homework,” said Ferguson.

A few hours later she checked her LinkedIn account. Their posts had been shared by dozens of people, with many sympathetic comments from strangers. Crucially, Ferguson could see that employees of CareFirst BlueCross BlueShield had seen it.
In early August, she received a surprising call from the insurer. “Good news!” the caller said. “We are going to approve your Keytruda.”
Ferguson said she wanted to scream: “What do you mean, good news?! For what?! For putting my life at risk by denying me the coverage that I need?! I’m in this situation because of you!” Instead, she thanked the caller, hung up and immediately scheduled her next infusion.
In December 2025, not long before Christmas, Ferguson received a new denial letter. She was now ready to give up. “I’m tired,” she thought at the time. But the reasons for the denial were so vague, she said — the insurance company sent a letter citing the 24-month limit and attached more than 15 pages of information about approved uses of Keytruda — that her health care provider said they would appeal. The denial was soon reversed, and she is back on Keytruda.
“I understand why some patients would give up,” she said. “You have to fight so hard because they deny you the medication that is keeping you alive. And for what? Just to save some money?”
Contributors: Violeta Santiago (Quinto Elemento Lab), Francisca Skoknic (LaBot), Guilherme Waltenberg (Poder360), Kathleen Cahill, Isabella Cota, Jesús Escudero, Sydney P. Freedberg, Karrie Kehoe and Nicole Sadek (ICIJ)
Source link
-

-

-

-

-




